
1911 Upper Arm and Shoulder Pathology: Tennis Elbow
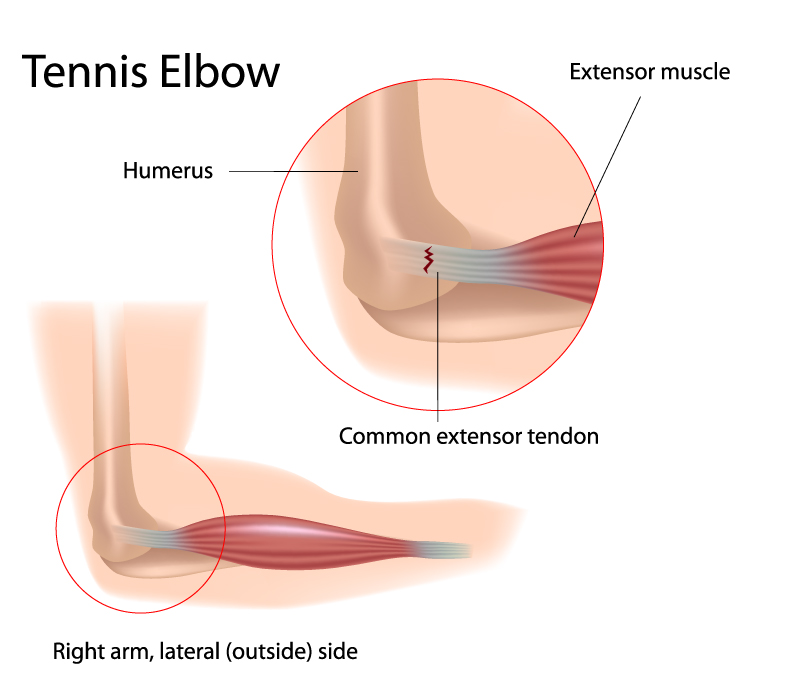
The image depicts a condition commonly known as Tennis Elbow, highlighting the lateral (outside) side of the right arm. The elbow joint, where this condition is focused, involves the distal end of the humerus, the upper arm bone, which is labeled at the top left.
Central to this condition is the common extensor tendon, depicted in the enlarged area. This tendon anchors the extensor muscles, which are responsible for extending the wrist and fingers, to the lateral epicondyle of the humerus. The image shows a zoomed-in view of the elbow where we can observe the extensor muscles transitioning into the common extensor tendon, indicating the point of convergence of these muscles before they attach to the bone.
The common extensor tendon is shown with a series of red and white striations near its attachment point, symbolizing the typical microtears and degeneration associated with Tennis Elbow. This injury is often due to repetitive motion or overuse, particularly gripping activities.
The condition’s name, Tennis Elbow, arises from its prevalence among tennis players. However, it can affect anyone who engages in activities that put a strain on the extensor muscles and tendons of the forearm.
The surrounding anatomy, including the humerus and the muscles of the forearm, are not the primary focus here but serve as a reference point to understand the location and impact of the condition on the arm’s structure and function.
When examining the condition of Tennis Elbow, it’s important to integrate our understanding of the arm’s anatomy to provide context for these considerations. The elbow joint itself is a complex structure involving the articulation of the humerus with the ulna and radius. In the case of Tennis Elbow, the extensor muscles on the lateral side of the forearm play a significant role. Overuse or repetitive motion can lead to the degeneration of the common extensor tendon, which is crucial for wrist and finger extension.
In terms of vascular supply, while not directly implicated in Tennis Elbow, the brachial artery’s continuation into the radial and ulnar arteries does supply blood to the forearm muscles. Any condition affecting the elbow could potentially influence or be influenced by the vascular supply, particularly during the healing process after injury or strain.
From a musculoskeletal perspective, the interosseous membrane and other connective tissues provide structural integrity to the forearm. While these structures are not directly involved in Tennis Elbow, their overall health and functionality can impact recovery and rehabilitation, as they support the muscles and tendons in question.
Lastly, understanding the nerve supply is also pertinent. Although Tennis Elbow primarily affects the tendons and muscles, any swelling or changes in the area could potentially affect nearby nerves. Given that the ulnar and median nerves provide the nerve supply to the forearm, careful consideration during the management of Tennis Elbow is necessary to avoid any nerve compression or injury.
In conclusion, while Tennis Elbow focuses on the tendons and muscles, a comprehensive approach to treatment and rehabilitation should consider the arm’s vascular, nervous, and musculoskeletal systems, as they are interrelated and can affect the healing process and functional recovery.