
7201 Hand and Wrist Pathology: Dupuytren’s Contracture
Dupuytren’s contracture is a progressive hand condition that affects the palmar fascia, leading to finger contracture. This paper elucidates the anatomy and physiology behind Dupuytren’s contracture, details its symptoms and clinical presentation, and examines the various diagnostic and treatment options available.
Keywords: Dupuytren’s contracture, palmar fascia, finger contracture, hand deformity, diagnosis, treatment
1. Anatomy and Physiology
Dupuytren’s contracture is characterized by abnormal thickening and contraction of the palmar fascia, the layer of tissue that lies beneath the skin in the palm of the hand. This fibrous tissue extends into the fingers, providing stability and flexibility for hand movements (Hurst & Badalamente, 2000).
In Dupuytren’s contracture, fibroblasts in the palmar fascia proliferate excessively and produce a collagen-rich matrix that forms nodules and thickened cords. Over time, these cords can contract, pulling the fingers into a flexed position that is difficult to extend (Degreef, 2014). This pathological process primarily affects the ring and little fingers but can involve any digit.
2. Symptoms and Clinical Presentation
The clinical presentation of Dupuytren’s contracture varies with disease progression. Early in the disease, patients may notice thickening or pitting of the skin in the palm. As the disease advances, nodules and cords develop, eventually leading to contracture of the affected fingers (Hurst & Badalamente, 2000).
Patients often have difficulty straightening the affected fingers, which impacts hand function and the ability to perform daily activities. The disease progression is usually slow and painless, although some patients may report discomfort or tenderness associated with the nodules (Degreef, 2014).
3. Diagnosis and Treatment Options
The diagnosis of Dupuytren’s contracture primarily involves a physical examination and review of the patient’s medical history. During the examination, the physician looks for the presence of palpable nodules or cords in the palm and checks the degree of finger contracture. X-rays or other imaging tests are generally unnecessary but can be used to rule out other conditions, if needed (Hurst & Badalamente, 2000).
The goal of treatment for Dupuytren’s contracture is to slow disease progression, relieve symptoms, and improve hand function. Non-surgical interventions include splinting and physical therapy, although their effectiveness is still under debate. Oral or injected medication may be used to slow the progression of the disease or to dissolve the cord (Degreef, 2014).
When the disease significantly affects the hand function or the contracture is severe, surgical intervention becomes necessary. The type of surgery depends on the severity and location of the contractures and can range from fasciotomy, where the cord is divided, to fasciectomy, where the diseased tissue is removed (Hurst et al., 2009).
In the image below, we can see a common progression of Dupuytren’s Contracture where there is a thickening of the palmer fascia around the flexor tendons causing the fingers to permanently bend or contract. The ring finger is most commonly affected followed by the pinky. The condition usually progresses slowly starting with a hardened knot around the flexor tendon pad. Later stages of the condition show more folding of the fascia in the palm and a more severe contraction of the fingers to the point where they can no longer straighten.
One of the reasons for the bunching up of fascia is the change in the consistency and type of the collagen in the fascia fibers of the hand. In Dupuytren’s Contracture, the collagen changes from a Type I to a Type III consistency with the likely cause pointing to a genetic abnormality where the genes use a different type of protein associated with Type III collagen.

By Frank C. Müller, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=647743
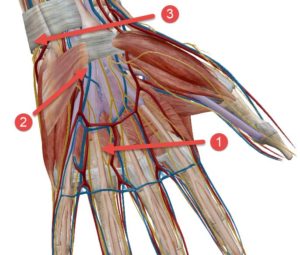
The treatment will start with the bunched up fascia near the base of the finger (1). Strike and place several times on a spot and feel for a change in tension. Check for a change in the movement of the finger over time as the fascia loosens. Then place the tuning fork on several spots on both sides of the tendon down the entire length from the base of the finger to the base of the palm (2). Keep checking for a change to the tension as you move across the hand.
There is also another phenomenon that we found to be associated with Dupuytren’s Contracture even at stages prior to the tendon becoming visible in the palm. Look for a hardened lump on the pinky side of the wrist (3). Place the tuning fork several times until you feel the lump soften or disappear.
Conclusion
Dupuytren’s contracture is a condition characterized by pathological changes in the palmar fascia, leading to finger contractures. Diagnosis involves a clinical examination, and treatment is tailored to the severity of the condition, ranging from non-surgical options to surgical interventions.
References
Degreef, I. (2014). How to treat the stiff finger? A review of the current options. Strategies in Trauma and Limb Reconstruction, 9(1), 1-6.
Hurst, L. C., & Badalamente, M. A. (2000). Dupuytren’s contracture. Journal of Hand Surgery, 25(4), 629-636.
Hurst, L. C., Badalamente, M. A., Hentz, V. R., Hotchkiss, R. N., Kaplan, F. T., Meals, R. A., Smith, T. M., & Rodzvilla, J. (2009). Injectable collagenase clostridium histolyticum for Dupuytren’s contracture. New England Journal of Medicine, 361(10), 968-979.